On the contrary, the huge majority feel covid less than the flu (hell, CDC is estimating 35% of infections dont even know they have it)You keep making the mistake that things would have been normal without any 'stay at home' orders. It's a bit hard to work when you're sick with COVID. With a common cold or even the flu one might even 'push through it' but with something this infectious you simply can't. Right now 1.19 million people - a new record - have it.

Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Map worldwide, with statistics
- Thread starter DIBBS
- Start date









- Status
- Not open for further replies.
Mark W
Gold $$ Contributor
On the contrary, the huge majority feel covid less than the flu (hell, CDC is estimating 35% of infections dont even know they have it)
The one person that I know who has tested positive thought he had a cold. He was required to be tested for his job and it came back positive. He lives in a household of five. He quarantined in one bedroom of the home and no one else got sick or tested positive even though there were no special precautions taken prior to his positive test.
How do you figure that? Protests have been going on for over 3 weeks now. Mean time to display symptoms is 5.5 days, so not only should the first wave be accounted for, we'd be in the middle of the contact cases now.Nah. That won’t kick in for another week or so.
Brians356
Silver $$ Contributor
"COVID-19 can take mild to severe courses: Sometimes there are no symptoms, and sometimes people die. New research suggests that blood types could play a rather important role by affecting the immune response. ... For a long time, COVID-19 research focused on high-risk patients: those who have certain preexisting conditions and/or have reached a certain age. Smokers also came under scrutiny as a potential high-risk group. Now, researchers are looking at a different piece in the coronavirus jigsaw puzzle."
https://www.dw.com/en/coronavirus-what-does-blood-type-have-to-do-with-covid-19/a-53869161-
https://www.dw.com/en/coronavirus-what-does-blood-type-have-to-do-with-covid-19/a-53869161-
On the contrary, the huge majority feel covid less than the flu (hell, CDC is estimating 35% of infections dont even know they have it)
The one person that I know who has tested positive thought he had a cold. He was required to be tested for his job and it came back positive. He lives in a household of five. He quarantined in one bedroom of the home and no one else got sick or tested positive even though there were no special precautions taken prior to his positive test.
An increasing number of people will have their own personal experiences. In my case, here in Miami a friend died several weeks ago after a long period in intensive care. I have many friends in Europe that have friends or relatives that have died. On the other hand I have two friends in Monaco who tested positive for antibodies - they were sick for about a week but fine after that. In another case here, a family of four, a friend of a close friend's brother came down with it. He died. As did her mother and father. They all died within three weeks of each other. I have a close friend who runs a landscaping business here in South Miami. This week, one of his crews came down with COVID. Three guys from the crew and one of their wives so far. He's just lost 20-25% of his workforce for at least two weeks, perhaps longer.
Do what you feel is right. But remember it's not just about you. In Florida, Texas, Arizona and several other states this thing is on the rampage, not coincidentally shortly after NPI were relaxed. We're still in the first wave. The last time a pandemic of this magnitude occurred it had three major waves and the second resulted in the most deaths. The trend in confirmed cases for the US overall has now turned back upwards.
Expanded and better prepared hospital capacity is already 85% full for normal beds and 86% full for ICU beds in Arizona and even more full in Florida. Indeed, the next couple of months will be interesting.
There's been some promising developments in treatment which hopefully will help the death rate although I'd not be at all be surprised if the current US toll more than doubled from here. At the very least a lot of people will be unwell with all the impact that will have. We are a year away from a vaccine.
The good news from an economic perspective is that the stimulus measures have been truly massive and there's nothing like a good crisis to weed out weak, inflexible, undercapitalized or over levered businesses and make the necessary restructurings in others. And in that regard everyone will have their own personal experience also: I don't have a single friend who hasn't continued to work through this crisis and so perhaps I should conclude that this has been the case for everyone else...
Be sensible. Just a suggestion.
ronsatspokane
Gold $$ Contributor
I know one person who died yesterday and one who will die Sunday (fathers day) when life support is disconnected after his teenage daughter has a chance to say goodbye. Neither are Covid related. No one gets out alive, make the best of the time you have.
One person at my wife's church died.The one person that I know who has tested positive thought he had a cold. He was required to be tested for his job and it came back positive. He lives in a household of five. He quarantined in one bedroom of the home and no one else got sick or tested positive even though there were no special precautions taken prior to his positive test.
A pastor I know was on a ventilator for a week.
I know a whole medical family (doctors and pharmacists) that contracted COVID-19 and wished they had died.
I don't know anyone who shook it off with just mild symptoms.
I know I'm still vulnerable because I had a blood test last week and don't have antibodies.
I'm being careful.
I don't know anyone who shook it off with just mild symptoms.
The variability of symptoms and effects seems to mark this virus out as being unusual if nothing else. Apart from range of effects during the active phase of the disease hearsay says there is a huge range of aftereffects too, often a long-lasting and very debilitating period of tiredness and loss of energy and stamina which is sometimes very severe. So, even those who are apparently only mildly affected while infected may need up to a couple of months recuperation afterwards before they can run their lives normally. Those so affected by aftereffects also report that it has a severe effect on their mental acuity and thought processes leading to poor decision making.
In the very early days of the disease when nobody knew nuttin as the saying goes about Coronavirus there was a lot of interest in the experiences of people on affected cruise liners, those modern plague ships. The BBC radio telephone interviewed a US citizen on board one who was a very early western country victim when it was still very much an Asian plague. He was a previously very active and fit 70 year old and his main phase was mild and confined him to bed for less than 48 hours after which all of the symptoms (dry cough, temperature, breathing difficulties) went completely. But, he was left so weak and with such effects on his joints and muscles that he was almost having to learn to walk again and was increasing his time on his feet and walking literally by a matter of 50 yards or so daily and it was apparent he'd take many weeks to regain his former fitness levels.
Here is a site that updates the numbers several times a day. It's scary how fast they are going up in the US.
https://www.worldometers.info/coronavirus/
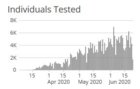
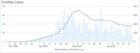
FYI link to Arizona dept of health COVID tracking. Note their graphics tend to be delayed vs their released data. For example Arizona has announced new confirmed cases in excess of 3k for two days in a row now while the graphic doesn't (as of this moment) include that data.
https://www.azdhs.gov/preparedness/...se-epidemiology/covid-19/dashboards/index.php
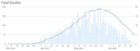
Note the climb in ICU bed utilization even though this will lag new case count significantly. Spare capacity of circa 250 beds doesn't seem like much when new cases are running at over 3k a day...
https://www.azdhs.gov/preparedness/...se-epidemiology/covid-19/dashboards/index.php
Note the climb in ICU bed utilization even though this will lag new case count significantly. Spare capacity of circa 250 beds doesn't seem like much when new cases are running at over 3k a day...
"COVID-19 can take mild to severe courses: Sometimes there are no symptoms, and sometimes people die. New research suggests that blood types could play a rather important role by affecting the immune response. ... For a long time, COVID-19 research focused on high-risk patients: those who have certain preexisting conditions and/or have reached a certain age. Smokers also came under scrutiny as a potential high-risk group. Now, researchers are looking at a different piece in the coronavirus jigsaw puzzle."
https://www.dw.com/en/coronavirus-what-does-blood-type-have-to-do-with-covid-19/a-53869161-
O it's so nice to be an O......
O it's so nice to be an O......
Exactly, if it's so. Everyone with this covid 19 crap that think they know so much couldn't hit themselves in their butts with both hands.
We're doomed.
By the very nature of a virus w/ a ~ 35% asymptomatic rate, the odds of you knowing someone who just "shook" it off are low because they never knew they had it. Which is entirely my point.One person at my wife's church died.
A pastor I know was on a ventilator for a week.
I know a whole medical family (doctors and pharmacists) that contracted COVID-19 and wished they had died.
I don't know anyone who shook it off with just mild symptoms.
I know I'm still vulnerable because I had a blood test last week and don't have antibodies.
I'm being careful.
Curious how you rationalize states that have relaxed policies (or never even shutdown entirely) where cases are continuing to drop.Do what you feel is right. But remember it's not just about you. In Florida, Texas, Arizona and several other states this thing is on the rampage, not coincidentally shortly after NPI were relaxed. We're still in the first wave. The last time a pandemic of this magnitude occurred it had three major waves and the second resulted in the most deaths. The trend in confirmed cases for the US overall has now turned back upwards.
When looking at rises in cases, you need to also look the % of positive tests coming back - many states that fall into "rising or flat" case count category has % that is falling. It stands to reason, the more testing becomes widespread and prevalent, the higher the case counts will be. And just to head off the rebuttal, im not saying increased testing is the only cause of rising cases. (but it is a factor).
Did you know yesterday the US had the least amount of covid deaths in a 24hr period since early March? In fact, death rates (if you can believe they are correctly attributed) continue to drop nationwide.
It seems that the current trend is cases increases but deaths stable or declining. Here is one such article:
https://slate.com/technology/2020/06/covid-death-rate-declining-explained.html
https://slate.com/technology/2020/06/covid-death-rate-declining-explained.html
Curious how you rationalize states that have relaxed policies (or never even shutdown entirely) where cases are continuing to drop.
When looking at rises in cases, you need to also look the % of positive tests coming back - many states that fall into "rising or flat" case count category has % that is falling. It stands to reason, the more testing becomes widespread and prevalent, the higher the case counts will be. And just to head off the rebuttal, im not saying increased testing is the only cause of rising cases. (but it is a factor).
Did you know yesterday the US had the least amount of covid deaths in a 24hr period since early March? In fact, death rates (if you can believe they are correctly attributed) continue to drop nationwide.
I've posted the data for Florida (flat testing rates with increasing positivity - quite different from simply more testing finding the same rate of positivity - and it now looks like the rate of hospitalizations may be turning upwards). And a link to Arizona's data. Feel free to add info for the others you feel strongly about. The healthcare system badly needed the time to provision in late March-April and later. Our business - we are in the healthcare equipment supply business - saw that extraordinary strain first hand. You really have no idea how poorly positioned hospitals and their staff were to handle intake of highly infectious patients. NPI provided a bit of a window for that equipping and planning to happen. The system, generally, is now better prepared, as I have said several times, but hospitalizations and deaths also lag rising case count figures. Note rising ICU bed occupancy in states such as Arizona, Texas and Florida. It will be interesting. Get it now while there's a bed free.
Also remember that sick people tend not to work or spend too much which impacts business and the economy.
Last edited:
I've posted the data for Florida (flat testing rates with increasing positivity - quite different from simply more testing finding the same rate of positivity - and it now looks like the rate of hospitalizations may be turning upwards). And a link to Arizona's data. Feel free to add info for the others you feel strongly about. The healthcare system badly needed the time to provision in late March-April and later. Our business - we are in the healthcare equipment supply business - saw that extraordinary strain first hand. You really have no idea how poorly positioned hospitals and their staff were to handle intake of highly infectious patients. NPI provided a bit of a window for that equipping and planning to happen. The system, generally, is now better prepared, as I have said several times, but hospitalizations and deaths also lag rising case count figures. Note rising ICU bed occupancy in states such as Arizona, Texas and Florida. It will be interesting. Get it now while there's a bed free.
Also remember that sick people tend not to work or spend too much which impacts business and the economy.
Again, how do you rationalize states that are continuing to open (or never locked down) where case rates are flat or falling (despite increased testing)?
You say hospitals were poorly positioned, yet the huge majority (I could say all except for a select few) never reached that poorly positioned capacity - how could they be poorly positioned if they never reached capacity? What you saw was a huge demand and limited supply, not a huge need.
Such as? Post your examples with numbers to support your arguments. I can think of many reasons that might apply.
The need for PPE was massive. Demand and need continues to be high (much of it are consumption items). Just think about the difference between admitting an infectious patient versus someone who is ill but their issues aren't transmitted to everyone around them. Ventilators were in high demand. Better to plan for more rather than find yourself short. Stocks are now better and are able to be redistributed to where they're needed most at any given time. The more difficult issue is planning bed capacity as adding this isn't as easy. A lot of additional bed capacity, some already planned and some not, was accelerated into service - to the extent that hospital finances allowed. Very big disparities here. Then of course there is the issue of having the requisite staff (and, again, why having adequate PPE is so important). Luckily NPI had the desired effect in the most critically affected States with consistent or lessening strain on resources. Need would have undoubtedly been a lot more without the breathing space provided. (Excuse the pun.) But also ICU bed utilization in States like Arizona, California and Florida is rising - unsurprisingly - with rapidly increasing case count. While one day doesn't make a trend, Florida today announced its second worse death count. (Arizona hit a record also.) Like I said, it's going to be interesting mostly because a belligerent population is unlikely to be sympathetic to renewed restrictions if hospital capacity is reached. We've just got to keep 'processing' the population through the virus, with its pruning - particularly - of over 60 year olds, until we get a vaccine in a year or so. Onwards!
The need for PPE was massive. Demand and need continues to be high (much of it are consumption items). Just think about the difference between admitting an infectious patient versus someone who is ill but their issues aren't transmitted to everyone around them. Ventilators were in high demand. Better to plan for more rather than find yourself short. Stocks are now better and are able to be redistributed to where they're needed most at any given time. The more difficult issue is planning bed capacity as adding this isn't as easy. A lot of additional bed capacity, some already planned and some not, was accelerated into service - to the extent that hospital finances allowed. Very big disparities here. Then of course there is the issue of having the requisite staff (and, again, why having adequate PPE is so important). Luckily NPI had the desired effect in the most critically affected States with consistent or lessening strain on resources. Need would have undoubtedly been a lot more without the breathing space provided. (Excuse the pun.) But also ICU bed utilization in States like Arizona, California and Florida is rising - unsurprisingly - with rapidly increasing case count. While one day doesn't make a trend, Florida today announced its second worse death count. (Arizona hit a record also.) Like I said, it's going to be interesting mostly because a belligerent population is unlikely to be sympathetic to renewed restrictions if hospital capacity is reached. We've just got to keep 'processing' the population through the virus, with its pruning - particularly - of over 60 year olds, until we get a vaccine in a year or so. Onwards!
What are you looking for examples of? States that continue to drop in case count despite more testing/ no lockdowns? I guess the most obvious one is Iowa - their gov was chastised relentlessly for not locking down, but their case count is flat/declining, while testing is increasing and the death rate continues to drop (they haven't had a single death the past 3 days)Such as? Post your examples with numbers to support your arguments. I can think of many reasons that might apply.
The need for PPE was massive. Demand and need continues to be high (much of it are consumption items). Just think about the difference between admitting an infectious patient versus someone who is ill but their issues aren't transmitted to everyone around them. Ventilators were in high demand. Better to plan for more rather than find yourself short. Stocks are now better and are able to be redistributed to where they're needed most at any given time. The more difficult issue is planning bed capacity as adding this isn't as easy. A lot of additional bed capacity, some already planned and some not, was accelerated into service - to the extent that hospital finances allowed. Very big disparities here. Then of course there is the issue of having the requisite staff (and, again, why having adequate PPE is so important). Luckily NPI had the desired effect in the most critically affected States with consistent or lessening strain on resources. Need would have undoubtedly been a lot more without the breathing space provided. (Excuse the pun.) But also ICU bed utilization in States like Arizona, California and Florida is rising - unsurprisingly - with rapidly increasing case count. While one day doesn't make a trend, Florida today announced its second worse death count. (Arizona hit a record also.) Like I said, it's going to be interesting mostly because a belligerent population is unlikely to be sympathetic to renewed restrictions if hospital capacity is reached. We've just got to keep 'processing' the population through the virus, with its pruning - particularly - of over 60 year olds, until we get a vaccine in a year or so. Onwards!
so are you qualifying your statement of 'poorly positioned' by referring only to PPE? Because, again, we saw a massive amount of orders for ventilators that never got used, we saw field hospitals built and torn down w/o seeing a patient, we saw hospitals across the country layoff/close because they were banned from performing "elective" operations and had no cash flow because they never saw the influx of covid patients. So much of the planning had negative consequences - arguably worse consequences than the virus itself.
The words used to describe the situation are very important, because it seems many news outlets, reps, etc. (even sales/supply agencies such as yourself) speak in absolutes, when that absolute (while very real) is only very real in isolated areas - particularly the major metro areas.
Attachments
Iowa? Are you serious? Population of just 3.2 million (a fraction of the greater Miami/Ft Lauderdale area) scattered over 56,272 square miles, a mere 56 people per square mile. Des Moines, the largest city, has a population of a mere 214k. A COVID carrier could probably walk around most of Iowa spitting and not infect anyone for days. Population density matters in human-to-human virus transmission. Maybe I missed something... 
Meanwhile in Texas... https://www.ft.com/content/30bed502-6fb9-4587-9254-93ffbda8cc5b
Some snippets:
- contingency plans being tested as doctors sound the alarm
- at Texas Medical Center which describes itself as "the largest medical center in the world" COVID patients in hospital are up 47% from a week ago
- in the two fullest public hospitals in Houston, Dr Persse (Houston's chief public health officer) described patients on stretchers in emergency department corridors, some forced to double up in rooms meant for one, and stressed nurses everywhere.
- Harris county, which includes Houston, could run out of existing intensive care beds in 11 days, on current trends, although surge capacity would be enough to manage for a further 27 days after that.
Meanwhile in Texas... https://www.ft.com/content/30bed502-6fb9-4587-9254-93ffbda8cc5b
Some snippets:
- contingency plans being tested as doctors sound the alarm
- at Texas Medical Center which describes itself as "the largest medical center in the world" COVID patients in hospital are up 47% from a week ago
- in the two fullest public hospitals in Houston, Dr Persse (Houston's chief public health officer) described patients on stretchers in emergency department corridors, some forced to double up in rooms meant for one, and stressed nurses everywhere.
- Harris county, which includes Houston, could run out of existing intensive care beds in 11 days, on current trends, although surge capacity would be enough to manage for a further 27 days after that.
Last edited:
- Status
- Not open for further replies.
Similar threads
- Replies
- 0
- Views
- 256
- Replies
- 238
- Views
- 13,086
Upgrades & Donations
This Forum's expenses are primarily paid by member contributions. You can upgrade your Forum membership in seconds. Gold and Silver members get unlimited FREE classifieds for one year. Gold members can upload custom avatars.

Click Upgrade Membership Button ABOVE to get Gold or Silver Status.
You can also donate any amount, large or small, with the button below. Include your Forum Name in the PayPal Notes field.
To DONATE by CHECK, or make a recurring donation, CLICK HERE to learn how.
Click Upgrade Membership Button ABOVE to get Gold or Silver Status.
You can also donate any amount, large or small, with the button below. Include your Forum Name in the PayPal Notes field.
To DONATE by CHECK, or make a recurring donation, CLICK HERE to learn how.